




![]()
Editor’s Note: Every Wednesday, James Hamblin takes questions from readers about health-related curiosities, concerns, and obsessions. Have one? Email him at paging.dr.hamblin@theatlantic.com.
Dear Dr. Hamblin,
I’m a college professor, but homeschooling my 6-year-old is proving to be one of the most challenging things I have ever done. I’m currently failing. Naturally, I have a lot of questions as schools are discussing reopening in the fall. A silver lining of this pandemic is that the disease seems to be mostly asymptomatic in children, but then, in May, I saw reports (and an advisory from the Centers for Disease Control and Prevention) about an inflammatory disease that was showing up in children. Can you explain how this is related to COVID-19, but isn’t considered COVID-19? And did it stop happening, or did we just stop hearing about it?
Jennifer Depold
Leander, Texas
The mysterious condition did seem to vanish, didn’t it? But unfortunately, it’s still happening, and it deserves serious attention.
The condition, known as Multisystem Inflammatory Syndrome in Children, or MIS-C, is distinct from COVID-19 (which kids can also get). It isn’t being monitored as closely or as comprehensively, so much is still unknown. Just this week in the New England Journal of Medicine, researchers reported that New York had seen 95 confirmed cases as of May 10. Some kids in New York and across the country have even died.
But these numbers are far from complete. The lack of such basic information comes down to the mysteries of this syndrome: The symptoms vary widely, and they may not appear right away. By the time they show up, many children test negative for the virus, but positive for antibodies. So it’s been difficult to prove that the virus is indeed the cause. Only in recent weeks have patterns become clear enough, around the world, to speak with much certainty.
At first, kids seemed to be mostly spared from the effects of the coronavirus. But in April, a few weeks after the initial surge in COVID-19 in the United States, strange cases started popping up in news reports and medical journals. The next month, the CDC warned parents, in a not-reassuring fashion, to consult a doctor “right away” if their child develops “symptoms of MIS-C” that include: “fever, abdominal pain, vomiting, diarrhea, neck pain, rash, bloodshot eye, [or] feeling extra tired.” This recommendation amounts to Call your doctor if anything happens at all.
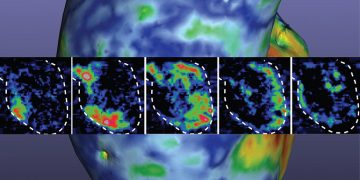
Since the initial news in the spring, physician groups have tried to define the syndrome more clearly. In a new review article in the journal Radiology, doctors in the U.K. report rapidly progressing inflammation in the lungs and abdomen of kids with MIS-C. Other children had blood clots and heart failure. The American College of Rheumatology recently noted that some children with MIS-C are in shock and have neurologic symptoms. They are also likely to develop an irregular heartbeat or to have their ventricles misfire, dangerously dropping their blood pressure. In some cases, kids have life-threatening aneurysms that threaten to burst the coronary arteries, the delicate vessels that supply blood to the heart.
[Read: Why the coronavirus hits kids and adults so differently]
But unlike COVID-19, these symptoms may take many weeks to show up in kids. When the CDC first warned about this syndrome, my colleague Sarah Zhang wrote a fascinating article explaining why the delay in identifying MIS-C was so dramatic. COVID-19 and MIS-C both can involve a serious immune-system dysfunction known as a cytokine storm. The process seems to be triggered by the coronavirus in both ailments, but it happens on different time scales. When adults come down with a severe case of COVID-19, their immune system goes into overdrive and crashes within days or weeks of contracting the coronavirus. Because this same crash rarely happens in kids, it initially seemed like they were mostly not harmed by the virus. But it seems now that some immune effects just take longer to show themselves.
The idea of an infectious microbe causing a delayed condition isn’t new. Polio can cause paralysis that comes on years after the virus has left the body, and strep throat can lead to rheumatic heart disease after the bacterial invasion subsides. When doctors first started reporting MIS-C, some assumed that they were seeing another type of immune reaction, known as Kawasaki disease. Only in recent weeks have physician groups started to reach a consensus that what’s happening is indeed unique to kids who’ve had the coronavirus.
Still, much beyond that remains unknown. For example, we still aren’t able to predict which kids will get MIS-C and which won’t. (The syndrome does seem to be more common in Black and Latino children than in white children.) Symptoms also might not show up for many months, conceivably, meaning more cases could emerge than current rates suggest. The coronavirus is still new to us, and this possibility can’t be ruled out until we’ve lived with it for much longer than we have.
The good news is that treating MIS-C seems to be doable, mostly with corticosteroids (what we colloquially call steroids) to tamp down the overactive immune system—a tried-and-true practice in medicine for decades. The burden of this condition will fall heavily on people who don’t have the means to get treated. Expanding access to health care is a solvable challenge.
[Read: The kids aren’t all right]
Ultimately, the ways to prevent this syndrome from happening are also not mysterious. As with so many other problems in this pandemic—medical and societal—what we have to do is limit the spread of the coronavirus. That means the same simple recommendations we’re all tired of hearing about: wash your hands, wear a mask, and continue social distancing.
Besides preventing kids themselves from getting MIS-C and COVID-19, the other reason to prevent transmission is the possibility that children can pass the coronavirus to adults, who are much more likely to get severely sick or die. The risk of children passing on the coronavirus is what makes it so difficult to consider reopening schools and day cares simply by counting the number of pediatric illnesses. It’s a reminder that nearly every decision in this pandemic involves a series of costs and benefits that might not be immediately apparent, or even yet known to science.
Until we know more, a safe assumption is that the virus is affecting more children than we currently realize. Hopefully that proves wrong, and cases remain rare and treatable. But more than 500,000 people have now died of COVID-19 around the world. The bigger mistake would be to unduly downplay MIS-C and overlook something serious amid the chaos.
“Paging Dr. Hamblin” is for informational purposes only, does not constitute medical advice, and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. By submitting a letter, you are agreeing to let The Atlantic use it—in part or in full—and we may edit it for length and/or clarity.
Related Podcast
Listen to James Hamblin discuss this column on an episode of Social Distance, The Atlantic’s guide to the pandemic:
Subscribe to Social Distance on Apple Podcasts or Spotify (How to Listen)